
The 30-Day Window That Defines Your Readmission Numbers
For hospital quality teams across Texas, the math hasn’t gotten any easier. CMS’s Hospital Readmissions Reduction Program (HRRP) keeps the pressure on; CHF and COPD remain two of the most penalized diagnoses, and the first 30 days after discharge still account for the bulk of avoidable returns to the emergency department.
If you’re a case manager, discharge planner, quality director, or utilization review lead in a Texas health system, you don’t need another lecture on why readmissions matter. You need a working playbook for what to actually do differently, especially for the two patient populations most likely to bounce back: congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD).
This piece breaks down the structural reasons these patients return, the five intervention windows that move the numbers, and where a virtual provider-oversight partner like Advanced Practice Health Connect (APHC) fits inside the workflow.
Why CHF and COPD Patients Drive So Many Readmissions
Both populations share a common pattern: clinical fragility, multiple medications, oxygen or respiratory device dependence, and slow recognition of decompensation at home.
CHF patients are usually readmitted because of:
- Diuretic non-adherence or under-dosing
- Sodium intake spikes
- Missed daily weight tracking
- Delayed identification of fluid overload
- Unfilled or wrong-dosed prescriptions after discharge
COPD patients are usually readmitted because of:
- Inhaler technique errors
- Late recognition of exacerbation symptoms
- Improper oxygen titration at home
- Missed pulmonary rehab connection
- Lack of a clear escalation pathway short of 911
What unites both lists is that nearly every cause is detectable with structured clinical follow-up within the first 7–14 days post-discharge, not 30, not 45.
The Five Most Common Reasons Discharges Fail
Across the systems APHC partners with in Texas and Oklahoma, the same five breakdowns repeat:
- The first follow-up visit is scheduled too late: A “two-week PCP follow-up” is often when the readmission happens, not when it gets prevented.
- Medication reconciliation never happens after discharge: What the patient is actually taking at day 5 frequently doesn’t match the discharge summary.
- The home health agency and the provider aren’t talking: Notes go out, but no one is closing the clinical loop.
- Respiratory support is set up but not supervised: Oxygen and CPAP arrive at the home; clinical oversight of their effective use does not.
- The patient has no clear, named clinician owning the 30 days. The hospitalist is done. The PCP isn’t engaged yet. The home health nurse covers the visit list but isn’t writing orders.
A successful 30-day readmission reduction program isn’t about working harder; it’s about closing those five gaps, every single discharge.
A Structured 30-Day Intervention Framework
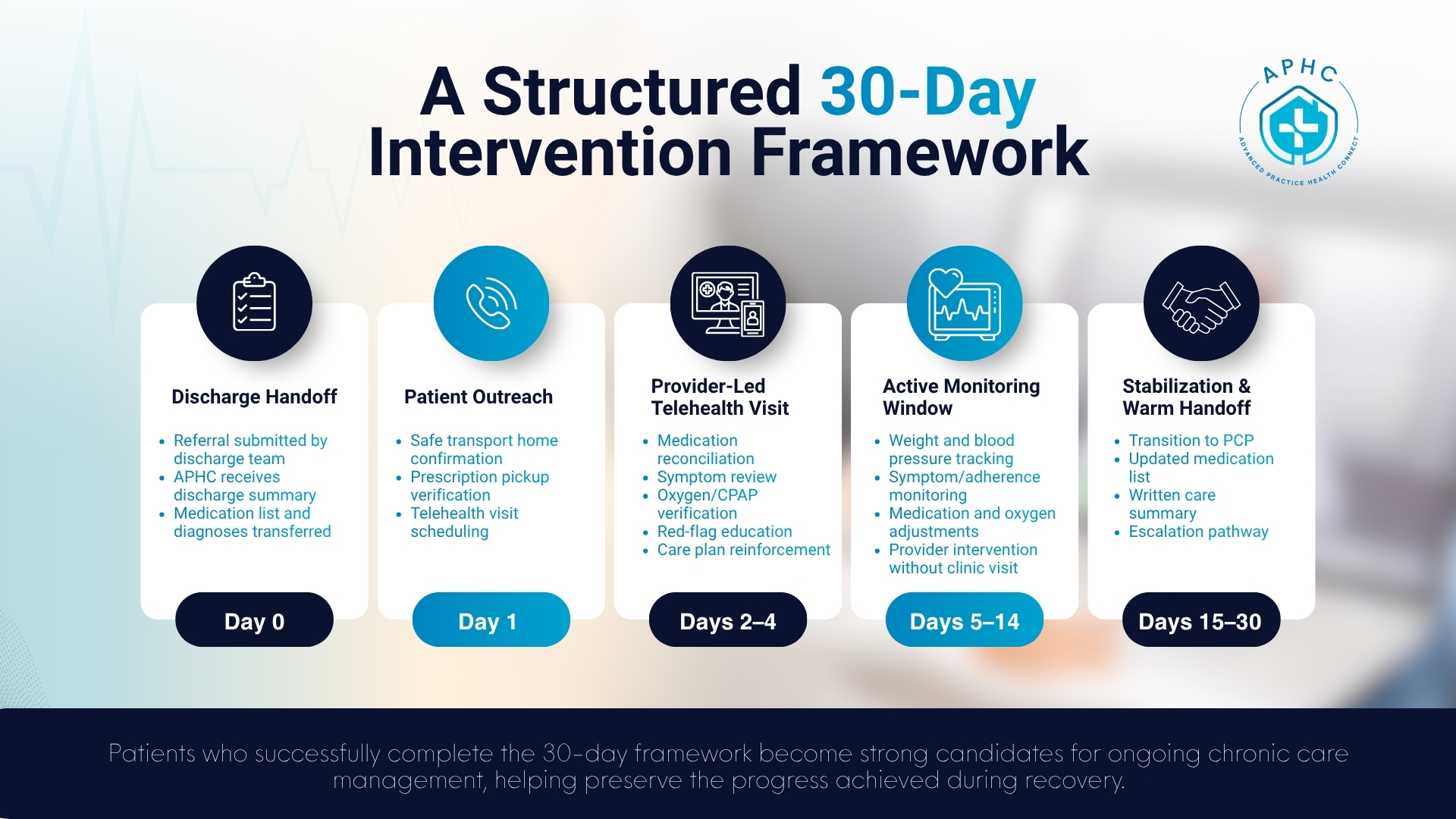
This is the framework APHC builds with hospital partners. Each step is a real, billable, documentable touchpoint.
Day 0 Discharge handoff: The discharging team submits a referral. APHC receives the discharge summary, medication list, and discharge diagnoses.
Day 1 (within 24 hours) Patient outreach: A care coordinator reaches the patient by phone, confirms safe transport home, verifies prescription pickup, and books the telehealth visit.
Days 2–4 Provider-led telehealth visit: A board-certified advanced practice provider performs a structured post-discharge evaluation: medication reconciliation, symptom review, oxygen/CPAP setup verification, red-flag teaching, and care plan reinforcement.
Days 5–14 Active monitoring window: Weight, blood pressure, symptoms, and adherence are tracked. Diuretic, inhaler, or oxygen adjustments are made by the provider when needed without waiting for a clinic appointment.
Days 15–30 Stabilization and warm handoff: The patient is transitioned back to their primary care provider with a written summary, updated medication list, and a clear escalation pathway.
Patients who complete the full 30-day window within this framework also become strong candidates for ongoing chronic care management, which helps protect the gains the discharge team worked so hard to build.
Where Virtual Provider Oversight Fits Inside the Workflow
A virtual provider oversight partner doesn’t replace your case managers, your home health agency, or the patient’s PCP. It fills the specific clinical gap that those teams can’t always fill: rapid, provider-level decision-making in the first 14 days, delivered remotely.
APHC functions as a clinical extension of your discharge plan. Concretely, that means:
- Patient seen by an advanced practice provider via secure telehealth within 48 hours of discharge
- Medication reconciliation completed, documented, and shared back to your team
- Oxygen, CPAP, and respiratory device use are clinically verified
- Diuretic, antihypertensive, and inhaler regimens adjusted in real time
- Documentation aligned with CMS Transitional Care Management (TCM) billing requirements
- Communication loops closed with the patient’s home health agency and primary care provider
For systems operating across Dallas, Fort Worth, Plano, Frisco, Arlington, Irving, McKinney, and surrounding Texas and Oklahoma communities, the model is delivered without geographic constraints; every patient gets the same standard of post-discharge oversight regardless of zip code.
Metrics That Actually Move
When hospital partners measure the impact of structured virtual post-discharge oversight, the metrics that consistently move are:
- 30-day all-cause readmission rate (CHF, COPD)
- Time from discharge to first provider contact (target: <48 hours)
- Time from discharge to first clinical visit (target: <7 days)
- Percentage of discharges with completed medication reconciliation
- Percentage of discharges with documented TCM-compliant follow-up
The improvement isn’t from any single touchpoint; it’s from the fact that something clinical is happening every few days, by someone with prescribing authority, until the patient is stable.
What Hospital Partnership With APHC Looks Like in Practice
Partnership doesn’t require a system overhaul. The setup is straightforward:
- A referral pathway is established between your discharge team and APHC
- A simple intake form or EHR-integrated referral submits the patient
- APHC contacts the patient within 24 hours
- Clinical notes, medication updates, and discharge documentation flow back to your team
- A dedicated APHC point of contact is available to your case managers
Hospital systems retain full ownership of the patient relationship. APHC operates as the provider-level extension during the highest-risk window.
A Word for Quality Directors and Value-Based Care Leaders
If your system participates in Medicare Advantage shared-savings, ACO arrangements, or bundled-payment programs, the financial logic of structured 30-day oversight is straightforward: avoided readmissions, fewer ED visits, stronger HEDIS performance, and stronger CMS Star Ratings. The clinical and financial cases point in the same direction.
For CHF and COPD specifically, two of the most penalized HRRP cohorts, virtual provider oversight is one of the highest-leverage interventions available, because it directly addresses the specific failure modes (medication errors, respiratory mismanagement, late symptom recognition) that drive readmission for those diagnoses.
Partner With APHC for Structured Post-Discharge Oversight in Texas and Oklahoma
If your readmission numbers for CHF or COPD have plateaued or worse, climbed, the gap is almost certainly in the first 14 days, not in the patient. Closing that gap is what APHC was built for.
We work with hospital systems, home health agencies, and payer care management teams across Texas and Oklahoma to deliver structured post-discharge provider oversight that fits inside your existing workflow.
Call 866-367-7031 or contact APHC to set up a partnership conversation.
